💯
Repeated that with another

This is amazing 🤩
💯 correct. It boggles the mind
One of the most challenging goodbyes occurs when we love someone yet recognize the impossibility of establishing a healthy relationship with them. Remaining in the relationship means continuing to wait for changes that will never materialize, tolerating hurtful actions, accepting minimal effort, and losing ourselves in an attempt to avoid loss. Although departing will be painful, it will ultimately lead to healing. Conversely, staying will perpetuate the cycle of hurt, causing the wound to deepen. Sometimes, choosing to leave is not a reflection of a lack of love for the person, but rather a demonstration of self-love and self-care, which necessitates leaving with love. -Unknown

Absolutely true 💯
THIS IS WHY KNOWLEDGE IS THE ONLY WEAPON FOR ESCAPING THEIR GRIP.
What is so confusing is the way the narcissist takes some vulnerable thing you said or did in the relationship and turns it into a big deal. Like if you openly say something like you prefer to NOT drive a lot because of your nerves.
The narcissist will bring it up out of nowhere to deflect from their behaviors and you are left confused because while it is true, it doesn’t apply to the situation in the moment. At first you will want to defend yourself, and later you see the gaslight, and finally you see the disorder.
All that time you thought to yourself why is communication so hard? It’s because you are dealing with a person who can’t emotionally connect or care.and uses bits of truth and twists the narrative around to suit them in the moment. Keep healing survivors .💛
Follow the yellow brick road. Follow the yellow brick road. Follow, follow, follow, follow, follow the yellow brick road.
If you’re not Following me on Bluesky, why not? It’s useful information.
If your attorney, your involved mental health professionals, your GALs and Parenting Coordinators, are not Following me on Bluesky, why not?
Sometimes I skeet about diagnosis. Sometimes I skeet about dark personalities. Sometimes I skeet about the court-involved assessment. Everything I skeet about is court-custody and treatment related.
Droplets of information each day, like a gentle rain of knowledge into the parched desert of the family courts.
I do what I do. You do what you do. We’re both working toward exactly the same goal – protecting the child from child abuse by a pathological parent.
I’m not your warrior – you’re the warrior fighting to protect your child. I’m a clinical psychologist with knowledge that’s useful to you. I’m your weapon.
I’m headed into the AFCC to contact the Hydra. You can’t do that. I can and I am because I do something different. I’m a clinical psychologist not a parent. We’re both working for exactly the same goal – protecting the child from child abuse – differently.
Because we’re in different roles.
Part of my role as a doctor is to educate the patient – you – about the pathology you have in your family… and with your child… so that you, as a parent, can get a proper assessment that will return an accurate diagnosis and effective treatment plan… to fix things.
Courts and the legal system land on the wrong end-point. Courts and the legal system land on the Court’s custody decision. That’s the wrong end-point of consideration.
The healthcare system lands on treatment. That’s where we need to end up – with a treatment plan that fixes things and gives the child a normal-range childhood.
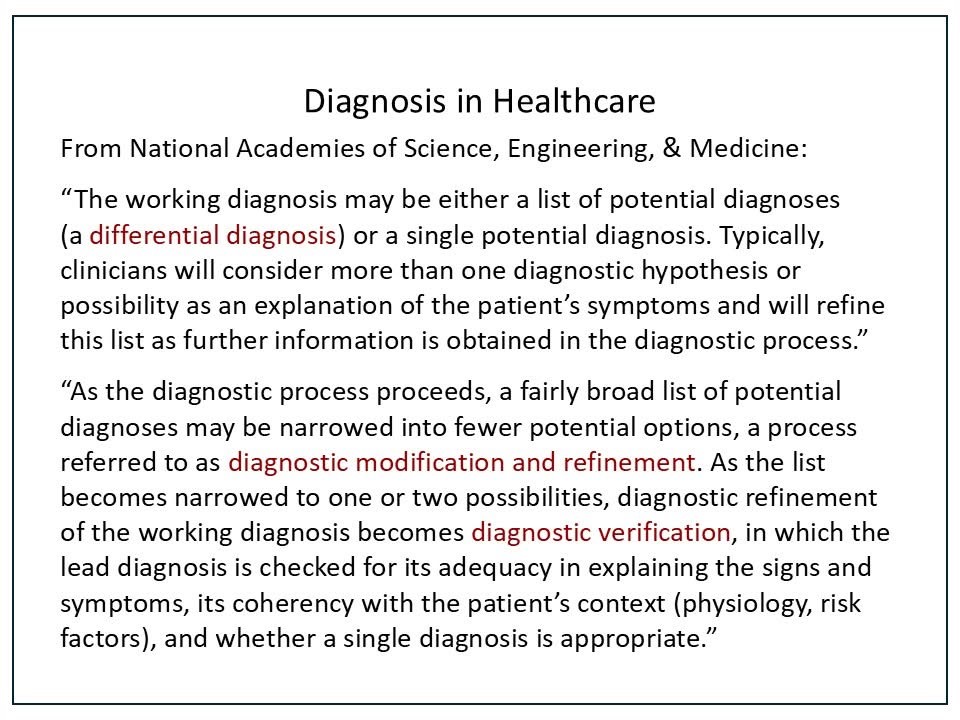
For a treatment plan… you’ll need a diagnosis. For an effective treatment plan, you’ll need an accurate diagnosis.
If we treat cancer with insulin because we think it’s diabetes, the patient will die from the misdiagnosed cancer. Whenever possible child abuse is a considered diagnosis, our returned diagnosis needs to be accurate 100% of the time.
Misdiagnosing child abuse is too devastating to the child. We need to get it right – every time. We can do that when there’s the motivation to to that.
The appellate system in healthcare for a disputed diagnosis is a second opinion, or even a third opinion. Doctors in healthcare consult all the time – because we need our diagnosis accurate and early – we need to start treatment right away.
Any diagnosis returned into the legal system will be a disputed diagnosis – so – let’s get a second or even third opinion right at the start through telehealth.
Get one primary treatment provider who will both diagnose and then treat the pathology. Allow each litigant parent to appoint a second-opinion doctor of their choice to represent their interests and concerns. Then let the doctors do what doctors do.
You’ll get a report from the primary treating doctor (duty of care) and two consulting reports that agree, or perhaps disagree to a degree. Provide this information to the Court for its decision-making.
The Court can decide which doctors make sense – and the doctors should make sense. They should 1) describe the symptoms, 2) describe the diagnostic criteria and established knowledge applied, and 3) the diagnosis that is supported by the symptom pattern.
Doctors are not concerned with custody. That’s the Court’s decision based on all the evidence it considers. There is NO quasi-judicial role for doctors. Doctors diagnose and treat pathology.
In the absence of child abuse, parents have the right to parent according to their cultural values, their personal values, and their religious values.
In the absence of child abuse, each parent should have as much time and involvement with the child as possible.
In the absence of child abuse, to restrict either parent’s time and involvement with the child would damage the child’s attachment bond to that parent, thereby harming the child and harming that parent.
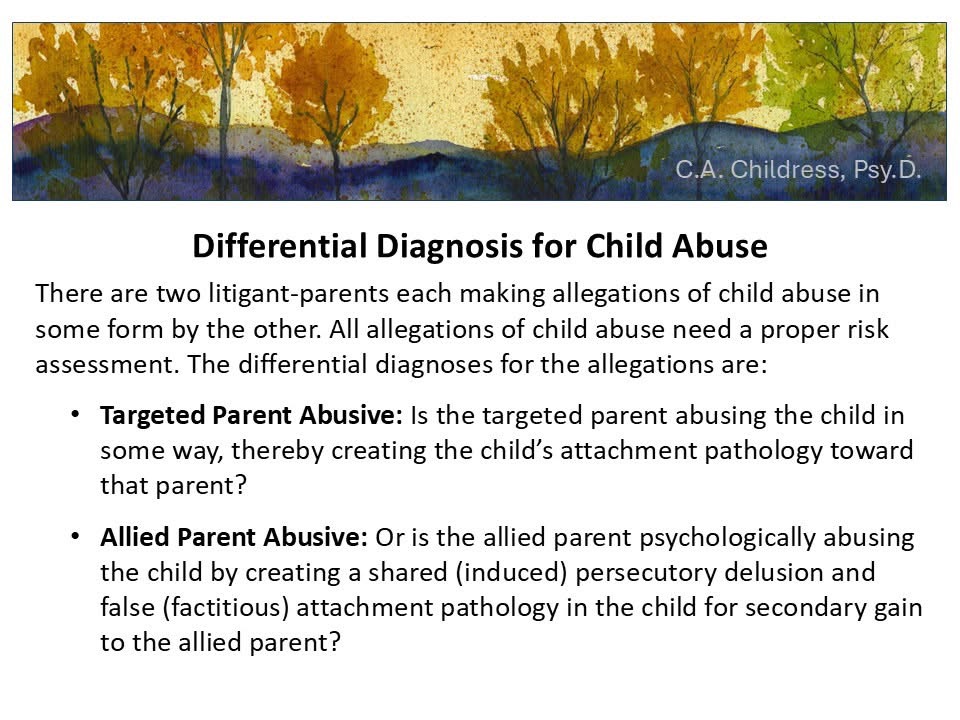
Is there child abuse? If a child is rejecting a parent, yes, there is child abuse by one parent or the other, we just don’t know which one yet.
It might be authentic child abuse by the targeted parent creating the child’s attachment pathology toward that parent – OR – it might be child psychological abuse by the allied parent who is creating a persecutory thought disorder and false (factitious) attachment pathology in the child for secondary gain to the parent.
Which parent is abusing the child? We need a proper risk assessment to the appropriate differential diagnoses for each parent to answer that question.
Then we protect the child. That’s what we do in ALL cases of child abuse. We always protect the child because ALL mental health professionals have a duty to protect in cases of three types of dangerous pathology – suicide – homicide – abuse (child, spousal, elder).
It’s not “complex” – it’s simple. What’s the diagnosis? Collect the symptom patterns, apply the diagnostic criteria patterns, and if there’s a pattern-match… that’s your diagnosis.
That’s not complex. That’s simple.
So is Following me on Bluesky. Sign up then Follow. Easy peasy for such valuable information to your professionals who surround you. Once they know… they can’t un-know what they know.
Craig Childress, Psy.D.
Clinical Psychologist
WA 61538481
OR 4392 – CA 18857