I’ve been thinking…
Now that I have the three DSM-5 Diagnoses seminars up on my YouTube channel, 1) the DSM-5 Diagnosis, 2) Diagnosing a Persecutory Delusion, and 3) Diagnosing a Factitious Disorder Imposed on the Child, I know what my next Diagnosis Chapter is…
4) Diagnosing Child Abuse
Because the forensic custody evaluators never diagnosed the child abuse – they never diagnosed anything, they do something different of their own devising – they put all the legal professionals to sleep… like things weren’t that important.
This is child abuse. We need an accurate diagnosis in six to eight weeks.
Which means the legal system must respond much-much more quickly… however we also need the psychologists to conduct the clinical diagnostic assessments.
Parents and the courts can ask for a diagnostic assessment of the family conflict as much as you want, if the psychologists don’t do that then it’s not available.
A diagnostic assessment is being withheld from parents and the courts for the personal financial gain of the forensic custody evaluators.
I’m in the AFCC now. I’ll be encountering the forensic custody evaluators there, and they’ll be encountering me.
Paradigms are changing. It’s not incremental change, it’s transformational change. Forensic custody evaluations are entirely leaving – bye-bye – a failed experiment on parents and children.
Clinical psychology is returning, diagnosis and treatment.
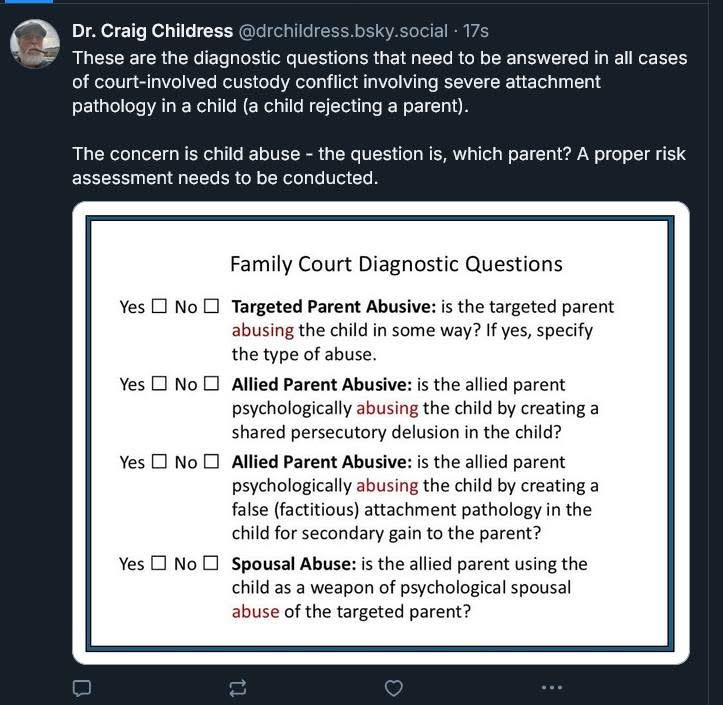
All mental health professionals have duty to protect obligations. This is child abuse – and spousal abuse of the targeted parent by the allied using the child, and the child’s induced pathology, as the spousal abuse weapon.
Duty to protect obligations are active – we need to get a proper risk assessment with an accurate diagnosis within six to eight weeks.
Since it will be a disputed diagnosis, each litigant-parent should be allowed to appoint a consultant to participate in the diagnostic assessment sessions through telehealth.
The ONLY cause of the child’s symptoms – a child seeking to flee a parent; a directional change in a primary motivational system – is child abuse by one parent or the other.
We need a clinical diagnostic assessment for child abuse to the appropriate differential diagnoses for each parent. How do we assess for child abuse?
That’s what I’ll explain in the next seminar: Diagnosing Child Abuse.
I served as the Clinical Director for a three-university assessment and treatment center for children ages 0-to-5 in foster care, CPS was our primary referral source.
I’ve personally treated all four forms of child abuse, and I have lead the treatment teams for all forms of child abuse that have included CPS social worker involvement.
I should describe how to assess for child abuse.
Craig Childress, Psy.D.
Clinical Psychologist
WA 71538481
OR 3942 – CA 18857