I’m a second opinion consultant. That’s what old folks are best at.
We have experience. The young do, the old consult from our accumulated wisdom.
I have a very niche role. I have a client-parent-attorney. My role is to do what I can to ensure the child and family receives an accurate diagnosis and effective treatment plan, and that the Court receives an accurate diagnosis of the family problem for its decision-making surrounding the child.
If you value my opinion regarding the pathology in the family, then I am of value. If my opinion regarding the pathology present in the family is not valued, then I am of no value.
It all comes down to my credibility. Is what I’m saying true or false?
Look it over. Decide. You’ll find that everything I say about the pathology in the family courts is 100% supported, true, and correct.
I know that. I know that it all comes down to credibility. That’s why I’ve grounded in established knowledge, beginning with the DSM-5 diagnostic system of the American Psychological Association and the ethics code for the American Psychological Association.
Forensic psychologists, take a look at what Dr. Childress is asserting. Is it true of false? Judges and court-involved professionals, take a look at what Dr. Childress is asserting. Is it true or false?
Decide. I’ll wait. Dum-dee-dum… it’s true.
So can we now move forward into protecting children from child abuse, and their parents from spousal abuse?
I wrote an email confirming the information I discussed in a consultation session with a parent for documentation purposes to be shared around professionals.
You may find it’s content helpful as well. I always say the same thing – and I’ll continue to say the same thing until we start protecting children from child abuse by a narcissistic-borderline-dark personality parent.
_______________
Diagnosis: your family will need an accurate diagnosis of the problem so that an effective treatment plan can be developed. Currently, I am not confident that the pathology (problem) in the family has been accurately diagnosed.
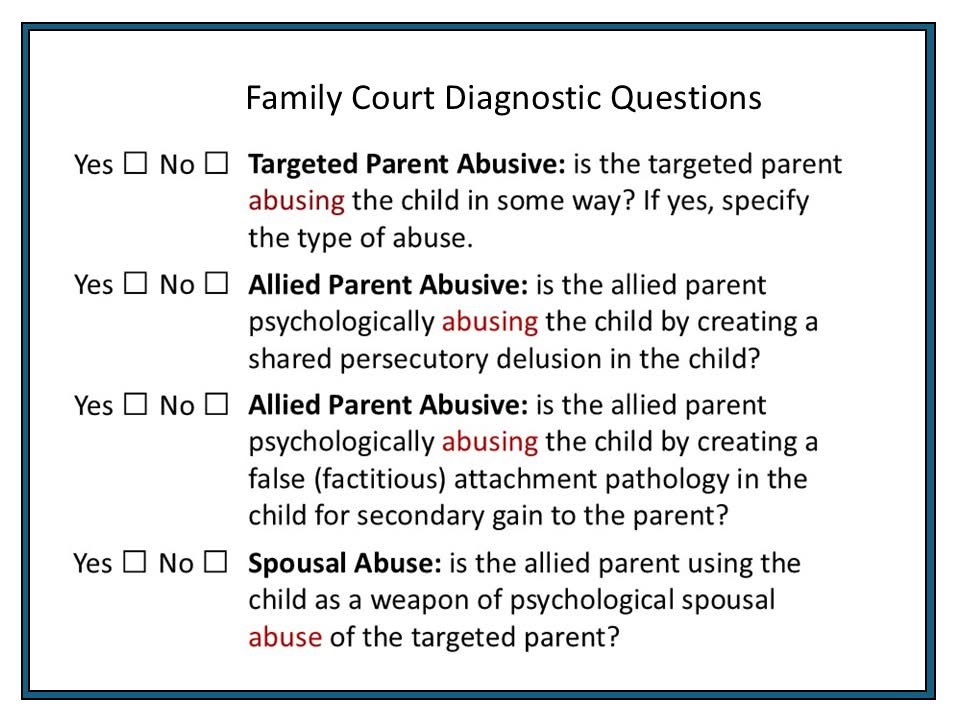
Clinical Concerns (differential diagnosis): the clinical concerns surrounding the family problem include the following differential diagnostic possibilities:
• Child abuse by father (specify the type of abuse)
• A persecutory delusion with the mother induced in the child (DSM-5 297.1 Delusional Disorder; persecutory type)
• A false (factitious) attachment pathology imposed on the child by the mother’s distorted parenting (DSM-5 300.19 Factitious Disorder Imposed on the Child; FDIA)
• Child psychological abuse by the mother who is creating false attachment pathology in the child for secondary gain to the mother (DSM-5 V995.51 Child Psychological Abuse)
• Spousal psychological abuse of the father by the mother using the children as the spousal abuse weapon (DSM-5 V995.82 Spouse or Partner Abuse, Psychological).
I have attached the diagnostic questions that need to be answered. The current family therapist has duty of care and duty to protect obligations relative to the diagnostic concerns involved.
I have the following resources available for the treating therapist and GAL (and Court) regarding the diagnostic assessment of court-involved family conflict surrounding child custody:
• YouTube Diagnosis Series: DSM-5 Diagnoses of Family Court Pathology
• YouTube Diagnosis Series: Diagnosing a Persecutory Delusion
• YouTube Diagnosis Series: Diagnosing a Factitious Disorder Imposed on the Child
• YouTube Diagnosis Series: Diagnosing Child Abuse in the Family Courts
• YouTube Diagnosis Series: Assessing Parenting
I recommend that a proper risk assessment be conducted for the family to the appropriate differential diagnoses for each parent. The current therapist has duty of care and duty to protect obligations, and it would be incumbent upon this therapist to either conduct a proper risk assessment for the dangerous pathologies potentially involved in the family, or to ensure that a proper risk assessment gets conducted.
Dangerous Pathology & Risk Assessments
There are three dangerous pathologies, suicide, homicide and abuse (child, spousal, and elder abuse), Whenever a mental health professional encounters any dangerous pathology (suicide, homicide, abuse) duty to protect obligations are active and the mental health professional must do three things:
1) Risk Assessment: the mental health professional must personally conduct a proper risk assessment for the danger involved, or ensure that a proper risk assessment gets conducted,
2) Protective Action: the mental health professional must take an affirmative protective action to ensure everyone’s safety (this might be increasing the frequency of sessions for a suicidal patient, or a CPS referral for child abuse concerns).
3) Documentation: the mental health professional should then document the findings of the risk assessment (if one was conducted) and the affirmative protective action taken.
I indicated that I am available for professional consultation with all court-involved mental health and legal professionals.
I am attaching the domains of my expertise and vita. Court-involved professionals can also follow me on Bluesky: @drchildress.bsky.social
Craig Childress, Psy.D.
Clinical Psychologist
WA 61538481
OR 3942 – CA 18857